Respiratory syncytial (sin-SISH-uhl) virus
ost clinical laboratories currently utilize antigen detection tests, and many supplement antigen testing with cell culture. Compared with culture, the sensitivity of antigen detection tests generally ranges from 80% to 90%. Antigen detection tests and culture are generally reliable in young children but less useful in older children and adults. Because of its thermolability, the sensitivity of RSV isolation in cell culture from respiratory secretions can vary among laboratories. Experienced laboratorians should be consulted for optimal results.
RT-PCR assays are now commercially available for RSV. The sensitivity of these assays often exceeds the sensitivity of virus isolation and antigen detections methods. Use of highly sensitive RT-PCR assays should be considered, particularly when testing older children and adults because they may have low viral loads in their respiratory specimens.
Serologic tests are less frequently used for routine diagnosis. Although useful for seroprevalence and epidemiologic studies, a diagnosis using paired acute- and convalescent-phase sera to demonstrate a significant rise in antibody titer to RSV cannot be made in time to guide patient care.
American Academy of Pediatrics (AAP) Guidelines for Infants and Children at Risk for Severe Illness Due to RSV Infection
According to the AAP1, palivizumab prophylaxis may be considered for the following infants and children
Infants born at 28 weeks’ gestation or earlier during RSV season, whenever that occurs during the first 12 months of life
Infants born at 29–32 weeks’ gestation if they are younger than 6 months of age at the start of the RSV season
Infants born at 32–35 weeks’ gestation who are younger than 3 months of age at the start of the RSV season or who are born during RSV season if they have at least one of the following 2 risk factors: 1) infant attends child care; 2) infant has a sibling younger than 5 years of age
Infants and children younger than 2 years with cyanotic or complicated congenital heart disease
Infants and children younger than 2 years who have been treated for chronic lung disease within 6 months of the start of the RSV season.
Infants born before 35 weeks of gestation who have either congenital abnormalities of the airway or neuromuscular disease that compromises handling of respiratory secretions

SmartMD (SACKIDMD) is 2 minutes of health update Follow @ Facebook.com/sackidMD or Twitter @ SackidMD. Resource from Dr. Prakasam's SACKID group.
Tuesday, January 31, 2012
Monday, January 30, 2012
PYLORIC STENOSIS
Pyloric stenosis is a narrowing of the pyloric outlet secondary to idiopathic hypertrophy of the pyloric muscle. It occurs in ~1/1000 births.
The male:female ratio is 5:1.
Infants usually present with vomiting
at 3-6 weeks of life.
The emesis is non-bilious and can be “projectile”.
If the vomiting is prolonged, the
infants can develop poor weight gain and dehydration (hypochloremic alkalosis). Diagnosis can be made clinically by history and physical exam. The hypertrophied pylorus can sometimes be palpated on abdominal exam (“olive”).
Pyloric sonograms and UGI series can also be helpful in making the
diagnosis.
Treatment is almost always surgical.
The male:female ratio is 5:1.
Infants usually present with vomiting
at 3-6 weeks of life.
The emesis is non-bilious and can be “projectile”.
If the vomiting is prolonged, the
infants can develop poor weight gain and dehydration (hypochloremic alkalosis). Diagnosis can be made clinically by history and physical exam. The hypertrophied pylorus can sometimes be palpated on abdominal exam (“olive”).
Pyloric sonograms and UGI series can also be helpful in making the
diagnosis.
Treatment is almost always surgical.
Sunday, January 29, 2012
Gower's sign

Duchenne muscular dystrophy is a rapidly-worsening form of muscular dystrophy. Other muscular dystrophies (including Becker's muscular dystrophy) get worse much more slowly.
Duchenne muscular dystrophy is caused by a defective gene for dystrophin (a protein in the muscles). However, it often occurs in people without a known family history of the condition.
Because of the way the disease is inherited, males are more likely to develop symptoms than are women. The sons of females who are carriers of the disease (women with a defective gene but no symptoms themselves) each have a 50% chance of having the disease. The daughters each have a 50% chance of being carriers.
Duchenne muscular dystrophy occurs in approximately 1 out of every 3,600 male infants. Because this is an inherited disorder, risks include a family history of Duchenne muscular dystrophy.
Duchenne muscular dystrophy - PubMed Health
Saturday, January 28, 2012
Calculating Absolute Neutrophil Count

White blood cell in thousands X percentage of Neutrophil
Example:
White blood cells = 3.8 = 3800 cells
Neutrophils = 12%
The ANC is 3800 x 12/100 = 456 THIS IS SEVERE NEUTROPENIA
Clinically Significant Neutrophil Counts
Clinically Significant Neutrophil Counts
ANC (Absolute Neutrophil Counts)
Clinical Significance
>1,500/mm3 Is Normal
1,000-1,500 No significant propensity to infection. Fevers can be managed on an outpatient basis.
500-1,000 Some propensity to infection. Occasionally fever can be managed on an outpatient basis.
less than 500 Significant propensity to infection. Always should be managed as inpatient with parenteral antibiotics. Few clinical signs of infection.
These rules apply strictly for neutropenia with hypoplastic marrow, early myeloid arrest, and decreased granulocyte reserve pools.
There is more latitude for clinical judgment in neutropenias with normocellular marrow.
The exception to these rules is chronic benign neutropenia of childhood.
ANC (Absolute Neutrophil Counts)
Clinical Significance
>1,500/mm3 Is Normal
1,000-1,500 No significant propensity to infection. Fevers can be managed on an outpatient basis.
500-1,000 Some propensity to infection. Occasionally fever can be managed on an outpatient basis.
less than 500 Significant propensity to infection. Always should be managed as inpatient with parenteral antibiotics. Few clinical signs of infection.
These rules apply strictly for neutropenia with hypoplastic marrow, early myeloid arrest, and decreased granulocyte reserve pools.
There is more latitude for clinical judgment in neutropenias with normocellular marrow.
The exception to these rules is chronic benign neutropenia of childhood.
Thursday, January 26, 2012
Adrenoleukodystrophy

X-ALD is an inherited metabolic storage disease whereby a defect in a specific enzyme results in the accumulation of very long-chain fatty acids (VLCFA) in tissues of the body, especially the brain and the adrenal glands. Ultimately the myelin sheath that surrounds the nerves is destroyed causing neurologic problems, and the adrenal gland malfunction causes Addison’s disease.
Symptoms normally start between the ages of 4 and 10 and include loss of previously acquired neurologic abilities, seizures, ataxia, Addison's disease, and degeneration of visual and auditory function.
Although there is no guaranteed method for preventing X-ALD, recommend genetic counseling for prospective parents with a family history of X-ALD. Female carriers can be diagnosed 85% of the time based on blood very long chain fatty acid (VLCFA) levels and genetic testing performed by specialized laboratories.
Prenatal diagnosis of X-ALD is also available. It is done by evaluating cells from chronic villus sampling or amniocentesis
Wednesday, January 25, 2012
Rheumatic Fever
Major criteria
§
Polyarthritis:
A temporary migrating inflammation of the large joints, usually starting in the
legs and migrating upwards.
§
Carditis:
Inflammation of the heart muscle which can manifest as congestive heart failure with shortness of breath, pericarditis with a rub, or a new heart murmur.
§
Subcutaneous nodules: Painless, firm collections
of collagen fibers over bones or tendons. They commonly appear on the back of
the wrist, the outside elbow, and the front of the knees.
§
Erythema
marginatum: A long lasting rash that
begins on the trunk or arms as macules and
spreads outward to form a snake like ring while clearing in the middle. This
rash never starts on the face and it is made worse with heat.
§
Sydenham’s chorea (St. Vitus’ dance): A characteristic series of
rapid movements without purpose of the face and arms. This can occur very late
in the disease for at least three months from onset of infection.
Minor
criteria
§
Fever of
38.2–38.9 °C (101–102 °F)
§ Neuralgia:
Joint pain without swelling (Cannot be included if polyarthritis is present as
a major symptom)
§
Raised erythrocyte sedimentation rate or C reactive protein
§
Leukocytosis
§
ECG showing
features of heart block, such as a prolonged PR interval (Cannot be included if carditis is present as a major
symptom)
§
First Degree AV-Block
§
Previous episode of rheumatic fever or inactive
heart disease


Tuesday, January 24, 2012
Erythema Nodusum


Erythema nodosum (EN) (red nodules) is an inflammation of the fat cells under the skin (panniculitis) characterized by tender red nodules or lumps that are usually seen on both shins. EN is an immunologic response to a variety of different causes.
Causes
In about 30-50% of cases, the cause of EN is unknown.
EN may be associated with a wide variety of diseases, including infections (e.g., hepatitis C, tuberculosis, streptococcal, Mycoplasma pneumoniae, Yersinia, and Epstein-Barr virus), Coccidioides immitis, sarcoidosis, autoimmune disorders (e.g., Inflammatory bowel disease or Behçet's disease), pregnancy, medications (sulfonamides, oral contraceptives, bromides), and cancer.
There is an association with the HLA-B27 histocompatibility antigen, which is present in 65% of patients with erythma nodosum.
Meningococcal vaccination - NEW recommendations
Administer a dose (a booster dose or the first dose if the adolescent is unvaccinated) after the 16th birthday and prior to college.
All college freshmen living in a dormitory are recommended to be fully vaccinated.
Only the meningococcal conjugate vaccine is recommended for adolescents. However, if the first dose of meningococcal vaccine was administered as polysaccharide vaccine, it is still counted as valid in the adolescent schedule. The booster dose of meningococcal vaccine for adolescents should always be a conjugate vaccine. The 2 licensed products, Menactra® and Menveo®, are interchangeable. If polysaccharide vaccine is inadvertently administered as the booster dose, revaccination with conjugate vaccine is recommended 8 weeks later.
All college freshmen living in a dormitory are recommended to be fully vaccinated.
Only the meningococcal conjugate vaccine is recommended for adolescents. However, if the first dose of meningococcal vaccine was administered as polysaccharide vaccine, it is still counted as valid in the adolescent schedule. The booster dose of meningococcal vaccine for adolescents should always be a conjugate vaccine. The 2 licensed products, Menactra® and Menveo®, are interchangeable. If polysaccharide vaccine is inadvertently administered as the booster dose, revaccination with conjugate vaccine is recommended 8 weeks later.
Monday, January 23, 2012
Celiac Disease Diagnosis


(courtesy - Gut doctor)
No screening test is perfect, and that the keys to confirming the diagnosis of CELIAC DISEASE remain a small intestinal biopsy combined with the patient’s subsequent clinical response to a gluten-free diet.
The tTG IgA ELISA test is highly sensitive and specific. The tTG assay correlates well with EMA-IgA and biopsy. TTG false positivity has been described in patients with both type I diabetes and autoimmune hepatitis. Theoretically, it can also be falsely positive in other autoimmune disease.
The antiendomysial IgA antibody is an excellent screening test for CELIAC DISEASE, with both a high sensitivity and specificity. It is considered the gold standard of antibodies. However, the subjective nature of this test (someone still needs to look at the slide under a microscope) may lead to false negative values and unacceptable variability between laboratories. Its major drawbacks are that it may be falsely negative in young children, in patients with IgA deficiency and a lesser degree of villous atrophy, and in the hands of an inexperienced laboratory.
CYSTIC FIBROSIS - DIAGNOSIS
Links: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1320177/ - The Relevance of Sweat Testing for the Diagnosis of Cystic Fibrosis in the Genomic Era
http://www.clsi.org/source/orders/free/c34-a3.pdf - approved guidelines for sweat chloride evaluation
Autosomal Recessive
Incidence: 1: 3200
Increased concentration of Sodium, Chloride and Potassium in their sweat
Diagnosis: Increased Sweat Chloride x 2 by pilocarpine iontotphoresis OR 2 CF mutations OR nasal epithelial ion transport
Sweat Chloride of more than 50mmol/litre or above need further evaluation
About 70% of mutations observed in CF patients result from deletion of three base pairs in CFTR's nucleotide sequence.



Sunday, January 22, 2012
Endocrine Society - Practice Guideline on Vitamin D 2011
Adults aged 19 to 70 years require at least 600 IU/day of vitamin D to maximize bone health and muscle function. However, getting 25(OH)D levels consistently above 30 ng/mL may require at least 1500 to 2000 IU/day of vitamin D.
Adults 70 years and older require at least 800 IU/day of vitamin D for bone health and fall prevention; at least 1500 to 2000 IU/day of supplemental vitamin D may be needed to keep 25(OH)D levels above 30 ng/mL.
Pregnant and lactating women need a minimum of 600 IU/day of vitamin D; 1500 IU/day may be needed to maintain blood levels of 25(OH)D higher than 30 ng/mL.
"Obese children and adults and children and adults on anticonvulsant medications, glucocorticoids, antifungals such as ketoconazole, and medications for AIDS need at least 2 to 3 times more vitamin D for their age group to satisfy their body's vitamin D requirement," Dr. Holick reported.
Tolerable upper limits of vitamin D, which "should not be exceeded without medical supervision," include the following:
1000 IU/day for infants aged up to 6 months,
1500 IU/day for infants aged 6 months to 1 year old,
2500 IU/day for children aged 1 to 3 years,
3000 IU/day for children aged 4 to 8 years, and
4000 IU/day for everyone older than 8 years.
However, the guideline states that for individuals who are vitamin D deficient, higher levels of vitamin D (2000 IU/day for children up to age 1 year; 4000 IU/day for children aged 1 - 18 years, and up to 10,000 IU/day for adults aged 19 years and older) "may be necessary to correct, treat, and prevent vitamin D deficiency,"

X-linked recessive inheritance
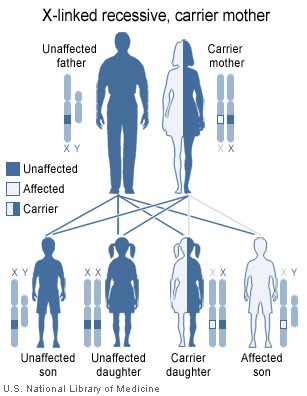
Usually,men are affected and women are carriers
SOME EXAMPLES
Color blindness
Hemophilia A
Duchenne muscular
dystrophy.
Becker's muscular
dystrophy;
Hemophilia B; a
blood clotting disorder caused by a mutation of the Factor IX gene, leading to
a deficiency of Factor IX. It is rarer than haemophilia A. It's also called
Christmas disease
X-linked
ichthyosis; a skin condition (ichthyosis)
X-linked
agammaglobulinemia
Glucose-6-phosphate
dehydrogenase deficiency
Dupuytren’s contracture

The cause is unknown.
One or both hands may be affected. The ring finger is affected most often, followed by the little, middle, and index fingers.
Treatment
Exercises, warm water baths, or splints may be helpful.
Surgery may be performed to release the contracture, depending on the severity of the condition. Normal movement of the fingers is usually restored by surgery followed by physical therapy exercises for the hand.
A newer treatment involves injecting a substance called collagenase into the scarred or fibrous tissue. Three injections are needed. You may have side effects such as swelling, pain, and itching. A more rare but severe side effect is rupture of the tendon.
Saturday, January 21, 2012

Clubbing of Fingers

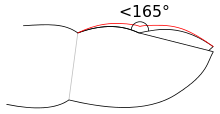
Clubbing develops in five steps:
- Fluctuation and softening of the nail bed (increased ballotability)
- Loss of the normal <165° angle (Lovibond angle) between the nailbed and the fold (cuticula)
- Increased convexity of the nail fold
- Thickening of the whole distal (end part of the) finger (resembling a drumstick)
- Shiny aspect and striation of the nail and skin
Schamroth's test or Schamroth's window test is a popular test for clubbing. When the distal phalanges (bones nearest the fingertips) of corresponding fingers of opposite hands are directly opposed (place fingernails of same finger on opposite hands against each other, nail to nail), a small diamond-shaped "window" is normally apparent between the nailbeds. If this window is obliterated, the test is positive and clubbing is present.
Prolactinoma is a benign tumor (adenoma)

A prolactinoma is a benign tumor (adenoma) of the pituitary gland that produces a hormone called prolactin. It is the most common type of pituitary tumor. Symptoms of prolactinoma are caused by too much prolactin in the blood (hyperprolactinemia) or by pressure of the tumor on surrounding tissues.
Prolactin stimulates the breast to produce milk, and has many other functions such as regulation of mood. Hence prolactin levels are usually higher during pregnancy and after childbirth. After delivery of a baby, a mother's prolactin levels come down to normal a few weeks after breastfeeding is discontinued. Each time the milk is dispensed, prolactin levels rise; this process may cycle to maintain milk production. In males it is responsible for the sexual refractory period after orgasm and excess levels can lead to erectile dysfunction.
Based on size, a prolactinoma can be classified as a microprolactinoma (<10 mm diameter) or macroprolactinoma (>10 mm diameter).
Trousseau sign

Trousseau sign of latent tetany is observed in patients with low calcium. This sign may become positive before other gross manifestations of hypocalcemia such as hyperreflexiaand tetany, but is generally believed to be more sensitive (94%) than the Chvostek sign (29%) for hypocalcemia.
To elicit the sign, a blood pressure cuff is placed around the arm and inflated to a pressure greater than the systolic blood pressure and held in place for 3 minutes. This will occlude the brachial artery. In the absence of blood flow, the patient's hypocalcemia and subsequent neuromuscular irritability will induce spasm of the muscles of the hand and forearm. The wrist andmetacarpophalangeal joints flex, the DIP and PIP joints extend, and the fingers adduct. The sign is also known as main d'accoucheur (French for "hand of the obstetrician") because it supposedly resembles the position of an obstetrician's hand in delivering a baby.
Chvostek sign
The Chvostek sign (also Weiss sign) is one of the signs of tetany seen in hypocalcemia. It refers to an abnormal reaction to the stimulation of the facial nerve. When the facial nerve is tapped at the angle of the jaw (i.e. masseter muscle), the facial muscles on the same side of the face will contract momentarily (typically a twitch of the nose or lips) because of hypocalcemia (i.e. from hypoparathyroidism, pseudohypoparathyroidism, hypovitaminosis D) with resultant hyperexcitability of nerves. Though classically described in hypocalcemia, this sign may also be encountered in respiratory alkalosis, such as that seen in hyperventilation, which actually causes decreased serum Ca2+ with a normal calcium level due to a shift of Ca2+ from the blood to albumin which has become more negative in the alkalotic state.
Friday, January 20, 2012
Maturity onset diabetes of the young (MODY)
Maturity onset diabetes of the young (MODY) - Now called Monogenic Diabetes
MODY 2 and MODY 3 are the most common forms. The severity of the different types varies considerably, but most commonly MODY acts like a very mild version of type 1 diabetes, with continued partial insulin production and normal insulin sensitivity. MODY is not type 2 diabetes in a young person, as might erroneously be inferred from the name.
MODY 2 and MODY 3 are the most common forms. The severity of the different types varies considerably, but most commonly MODY acts like a very mild version of type 1 diabetes, with continued partial insulin production and normal insulin sensitivity. MODY is not type 2 diabetes in a young person, as might erroneously be inferred from the name.
Treatment
In some forms of MODY, standard treatment is appropriate, though exceptions occur:
- In MODY2, oral agents are relatively ineffective and insulin is unnecessary.
- In MODY1 and MODY3, insulin may be more effective than drugs to increase insulin sensitivity.
The following characteristics suggest the possibility of a diagnosis of MODY in hyperglycemic and diabetic patients:
- Mild to moderate hyperglycemia (typically 130–250 mg/dl, or 7-14 mM/L) discovered before 30 years of age. However, anyone under 50 can develop MODY.
- A first-degree relative with a similar degree of diabetes.
- Absence of positive antibodies or other autoimmunity (e.g., thyroiditis) in patient and family.
- Persistence of a low insulin requirement (e.g., less than 0.5 u/kg/day) past the usual "honeymoon" period.
- Absence of obesity (although overweight or obese people can get MODY), or other problems associated with type 2 diabetes or metabolic syndrome (e.g. hypertension, hyperlipidemia, polycystic ovary syndrome).
- Insulin resistance very rarely happens.
Subscribe to:
Comments (Atom)